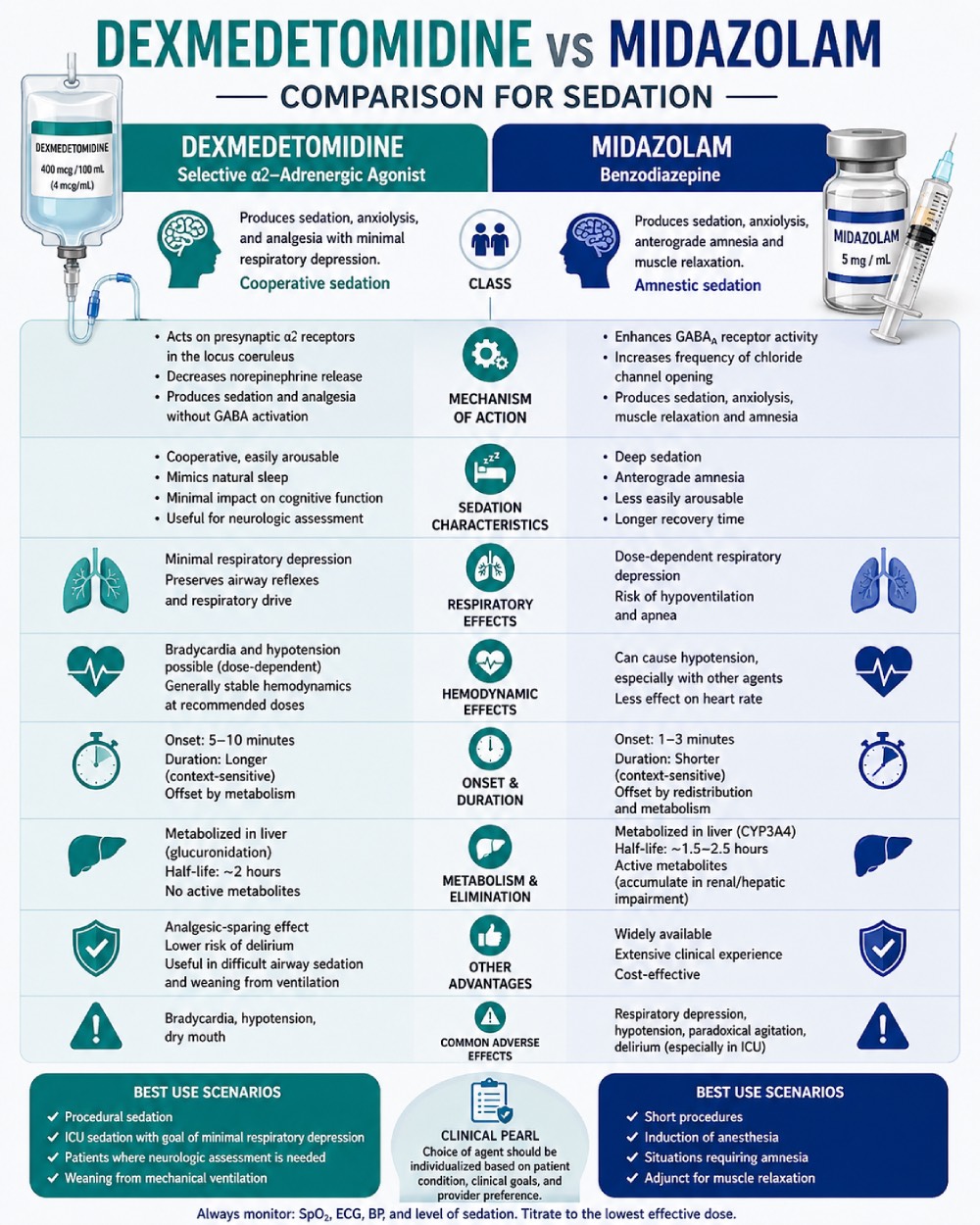
Sedation is a fundamental component of perioperative and critical care medicine, with drug selection critically influencing patient safety, comfort, and clinical outcomes. Midazolam, a benzodiazepine, is a standard agent for procedural sedation, valued for its rapid onset, anxiolytic properties, and amnestic effects. Dexmedetomidine, a highly selective α2-adrenoceptor agonist, offers sedative, analgesic, and anxiolytic effects without the respiratory depression classically associated with benzodiazepines. Research has identified advantages and disadvantages for dexmedetomidine and midazolam for procedural sedation in varying clinical contexts.
Eren et al. demonstrated that dexmedetomidine (1 µg/kg) provided sedation equivalent to, or greater than, midazolam at its highest studied dose (0.06 mg/kg), as measured by Ramsay sedation scores and visual analogue scores for anxiety¹. Notably, the sedative effect of dexmedetomidine persisted beyond the 30-minute observation window, whereas the effect of midazolam at 0.06 mg/kg had already begun to wane at 25 minutes, consistent with midazolam’s shorter effective duration. Dexmedetomidine produced significant reductions in mean arterial pressure and heart rate, but these changes did not reach clinically defined thresholds for hypotension or bradycardia and may in part represent normalization of elevated catecholamine levels attributable to preoperative anxiety¹.
Hemodynamic effects in anesthetic agents merit careful attention, given the precise hemodynamic control necessary for patient safety. In a pair of randomized controlled trials conducted across multiple European intensive care units, Jakob et al. reported that dexmedetomidine was non-inferior to both midazolam and propofol in maintaining target sedation levels in mechanically ventilated patients requiring prolonged sedation². However, dexmedetomidine was associated with significantly higher rates of hypotension (20.6% vs. 11.6%) and bradycardia (14.2% vs. 5.2%) compared with midazolam in the MIDEX trial².
These adverse hemodynamic effects must therefore be weighed against the agent’s clinical benefits, which include a significantly shorter duration of mechanical ventilation compared with midazolam, earlier time to extubation compared with both midazolam and propofol, and substantially improved patient arousability and ability to communicate pain to nursing staff².
A systematic review examining dexmedetomidine versus midazolam in procedural sedation across twelve clinical trials involving 883 patients found that dexmedetomidine was consistently associated with higher patient and clinician satisfaction scores compared with midazolam³. Patients receiving dexmedetomidine also reported lower pain scores and required less supplemental analgesia, a reflection of the drug’s intrinsic analgesic properties—properties that midazolam lacks, and which the latter may paradoxically counteract by lowering pain thresholds³.
Respiratory and hemodynamic safety profiles were broadly comparable between the two agents when both were carefully titrated, though the authors emphasized that this equivalence depends heavily on adherence to slow, controlled infusion protocols³. Though this deficit in midazolam may be addressed by incorporating analgesic agents into a patient’s anesthesia care, this may not be the optimal approach depending on the clinical situation.
The analgesic adjuvant role of dexmedetomidine extends to regional anesthesia as well. A meta-analysis by Niu et al., pooling data from eight randomized controlled trials involving 412 patients, demonstrated that both intravenous and intrathecal dexmedetomidine significantly prolonged the duration of sensory and motor block during spinal anesthesia and extended the time to first postoperative analgesic request by a mean of approximately 246 minutes⁴. The incidence of hypotension and other adverse events did not differ significantly from placebo; however, dexmedetomidine was associated with a substantially increased requirement for atropine to manage bradycardia⁴.
A comparative study in the setting of cataract surgery under peribulbar anesthesia provided an important counterpoint: despite dexmedetomidine producing slightly higher patient satisfaction with sedation compared with midazolam, it resulted in significantly delayed recovery room discharge (median 45 versus 21 minutes), owing to its longer elimination half-life of approximately two hours⁵. This finding carries meaningful implications for high-volume ambulatory surgical settings, where throughput and efficient recovery are operationally critical.
Dexmedetomidine represents a clinically valuable alternative to midazolam for procedural sedation. Its principal advantages include superior analgesic properties, preserved arousability, and reduced respiratory depression. Its principal limitations are a propensity for bradycardia and hypotension, and a prolonged duration of action that may delay discharge in ambulatory procedures.
References
- Eren, G. et al. Comparison of dexmedetomidine and three different doses of midazolam in preoperative sedation. J. Anaesthesiol. Clin. Pharmacol. 27, 367–372 (2011). https://doi.org/10.4103/0970-9185.83684
- Jakob, S. M. et al. Dexmedetomidine vs midazolam or propofol for sedation during prolonged mechanical ventilation: two randomized controlled trials. JAMA 307, 1151–1160 (2012). https://jamanetwork.com/journals/jama/fullarticle/1105080
- Barends, C. R. M. et al. Dexmedetomidine versus midazolam in procedural sedation. A systematic review of efficacy and safety. PLoS ONE 12, e0169525 (2017). https://doi.org/10.1371/journal.pone.0169525
- Niu, X.-Y. et al. Effects of intravenous and intrathecal dexmedetomidine in spinal anesthesia: a meta-analysis. CNS Neurosci. Ther. 19, 897–904 (2013). https://pmc.ncbi.nlm.nih.gov/articles/PMC6493572/
- Alhashemi, J. A. Dexmedetomidine vs midazolam for monitored anaesthesia care during cataract surgery. Br. J. Anaesth. 96, 722–726 (2006). https://doi.org/10.1093/bja/ael080